Copper deficiency
Copper deficiency, or hypocupremia, is defined either as insufficient copper to meet the needs of the body, or as a serum copper level below the normal range.[1] Symptoms may include fatigue, decreased red blood cells, early greying of the hair, and neurological problems presenting as numbness, tingling, muscle weakness, and ataxia.[2] The neurodegenerative syndrome of copper deficiency has been recognized for some time in ruminant animals, in which it is commonly known as "swayback".[3] Copper deficiency can manifest in parallel with vitamin B12 and other nutritional deficiencies.[2]
Copper deficiency
Overview[edit]
The most common cause of copper deficiency is a remote gastrointestinal surgery, such as gastric bypass surgery, due to malabsorption of copper, or zinc toxicity. On the other hand, Menkes disease is a genetic disorder of copper deficiency involving a wide variety of symptoms that is often fatal.[4]
Copper is required for the functioning of many enzymes, such as cytochrome c oxidase, which is complex IV in the mitochondrial electron transport chain, ceruloplasmin, Cu/Zn superoxide dismutase, and in amine oxidases.[3] These enzyme catalyze reactions for oxidative phosphorylation, iron transportation, antioxidant and free radical scavenging and neutralization, and neurotransmitter synthesis, respectively.[3] Diets vary in the amount of copper they contain, but may provide about 5 mg/day, of which only 20-50% is absorbed.[2] The diet of the elderly may have a lower copper content than the recommended daily intake.[2] Dietary copper can be found in whole grain cereals, legumes, oysters, organ meats (particularly liver), cherries, dark chocolate, fruits, leafy green vegetables, nuts, poultry, prunes, and soybean products like tofu.[5]
Copper deficiency can have many hematological consequences, such as myelodysplasia, anemia, low white blood cell count, and low count of neutrophils (a type of white blood cell that is often called "the first line of defense" of the immune system).[2] Copper deficiency has long been known as a cause of myelodysplasia (when a blood profile has indicators of possible future leukemia development), but it was not until 2001 that copper deficiency was associated with neurological manifestations like sensory ataxia (irregular coordination due to proprioceptive loss), spasticity, muscle weakness, and more rarely visual loss due to damage in the peripheral nerves, myelopathy (disease of the spinal cord), and rarely optic neuropathy.
Signs and symptoms[edit]
Blood symptoms[edit]
The characteristic hematological (blood) effects of copper deficiency are anemia (which may be microcytic, normocytic or macrocytic) and neutropenia.[6] Thrombocytopenia (low blood platelets) is unusual.[2][7]
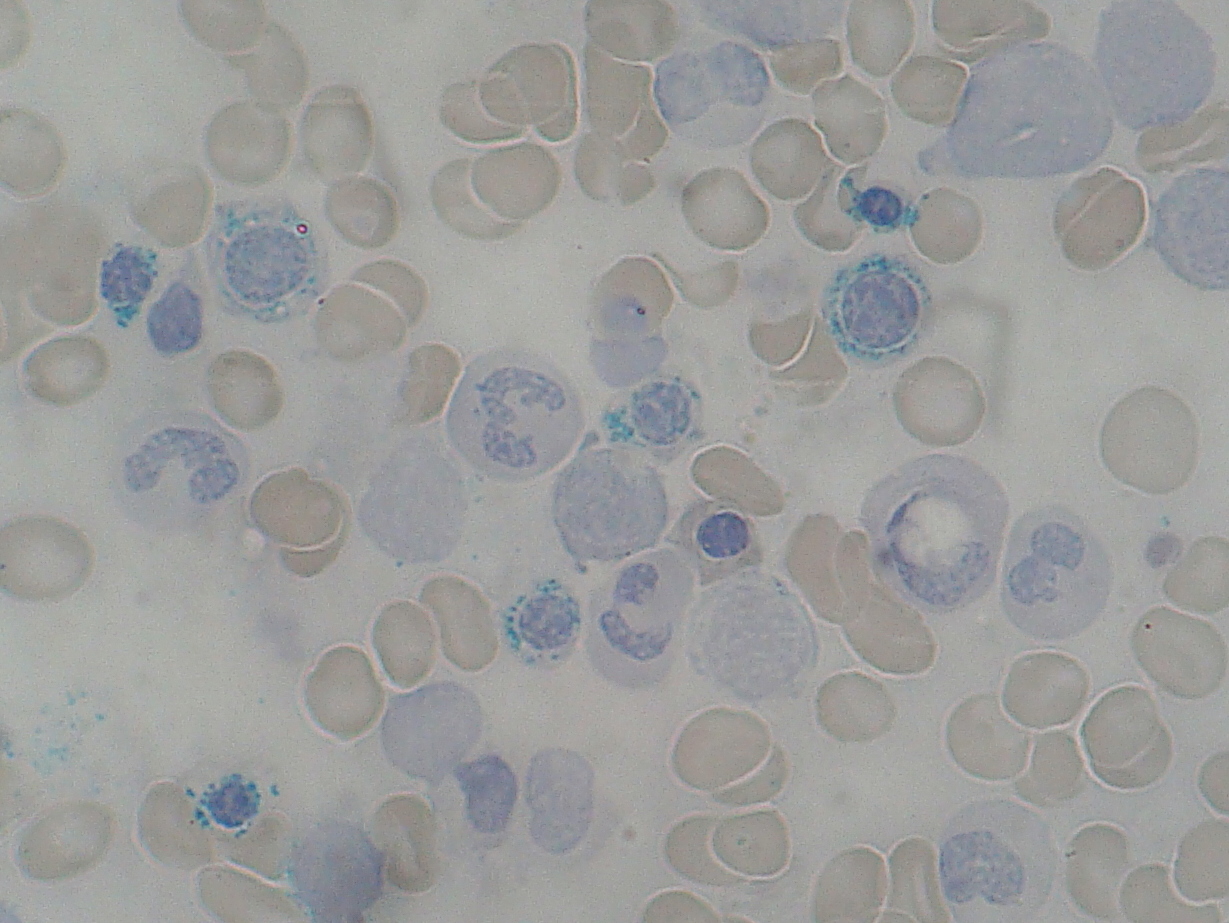
The peripheral blood and bone marrow aspirate findings in copper deficiency can mimic myelodysplastic syndrome.[8] Bone marrow aspirate in both conditions may show dysplasia of blood cell precursors and the presence of ring sideroblasts (erythroblasts containing multiple iron granules around the nucleus). Unlike most cases of myelodysplastic syndrome, the bone marrow aspirate in copper deficiency characteristically shows cytoplasmic vacuoles within red and white cell precursors, and karyotyping in cases of copper deficiency does not reveal cytogenetic features characteristic of myelodysplastic syndrome.[6][7]
Anemia and neutropenia typically resolve within six weeks of copper replacement.[8]
Neurological symptoms[edit]
Copper deficiency can cause a wide variety of neurological problems including myelopathy, peripheral neuropathy, and optic neuropathy.[3][7]
Causes[edit]
Surgery[edit]
Bariatric surgery is a common cause of copper deficiency.[3][6] Bariatric surgery, such as gastric bypass surgery, is often used for weight control of the morbidly obese. The disruption of the intestines and stomach from the surgery can cause absorption difficulties not only as regards copper but also for iron and vitamin B12 and many other nutrients.[3] The symptoms of copper deficiency myelopathy may take up to decades to develop.
Zinc toxicity[edit]
Increased consumption of zinc is another cause of copper deficiency.[7] Zinc is often used for the prevention or treatment of common colds and sinusitis (inflammation of sinuses due to an infection), ulcers, sickle cell disease, celiac disease, memory impairment, and acne.[7] Zinc is found in many common vitamin supplements and is also found in denture creams.[7][15][16] Recently, several cases of copper deficiency myeloneuropathy were found to be caused by prolonged use of denture creams containing high quantities of zinc.[15][16]
Metallic zinc is the core of all United States currency coins, including copper-coated pennies. People who ingest a large number of coins will have elevated zinc levels, leading to zinc-toxicity-induced copper deficiency and the associated neurological symptoms. This was the case for a 57-year-old woman diagnosed with schizophrenia. The woman consumed over 600 coins, and started to show neurological symptoms such as unsteady gait and mild ataxia.[17]
Diagnosis[edit]
The diagnosis of copper deficiency may be supported by a person's report of compatible signs and symptoms, findings from a thorough physical examination, and supportive laboratory evidence. Low levels of copper and ceruloplasmin in the serum are consistent with the diagnosis as is a low 24 hour urine copper level.[20] Additional supportive bloodwork findings also include neutropenia and anemia.[20] MRI imaging may demonstrate increased T2 signal of the dorsal column–medial lemniscus pathways.[20]
Treatment[edit]
Copper deficiency is a very rare disease and is often misdiagnosed several times by physicians before concluding the deficiency of copper through differential diagnosis (copper serum test and bone marrow biopsy are usually conclusive in diagnosing copper deficiency). On average, patients are diagnosed with copper deficiency around 1.1 years after their first symptoms are reported to a physician.[3] Copper deficiency can be treated with either oral copper supplementation or intravenous copper.[7] If zinc intoxication is present, discontinuation of zinc may be sufficient to restore copper levels back to normal, but this usually is a very slow process.[7] People with zinc intoxication will usually have to take copper supplements in addition to ceasing zinc consumption. Hematological manifestations are often quickly restored back to normal.[7] The progression of the neurological symptoms will be stopped and sometimes improved with appropriate treatment, but residual neurological disability is common.[20]