Embryonic stem cell
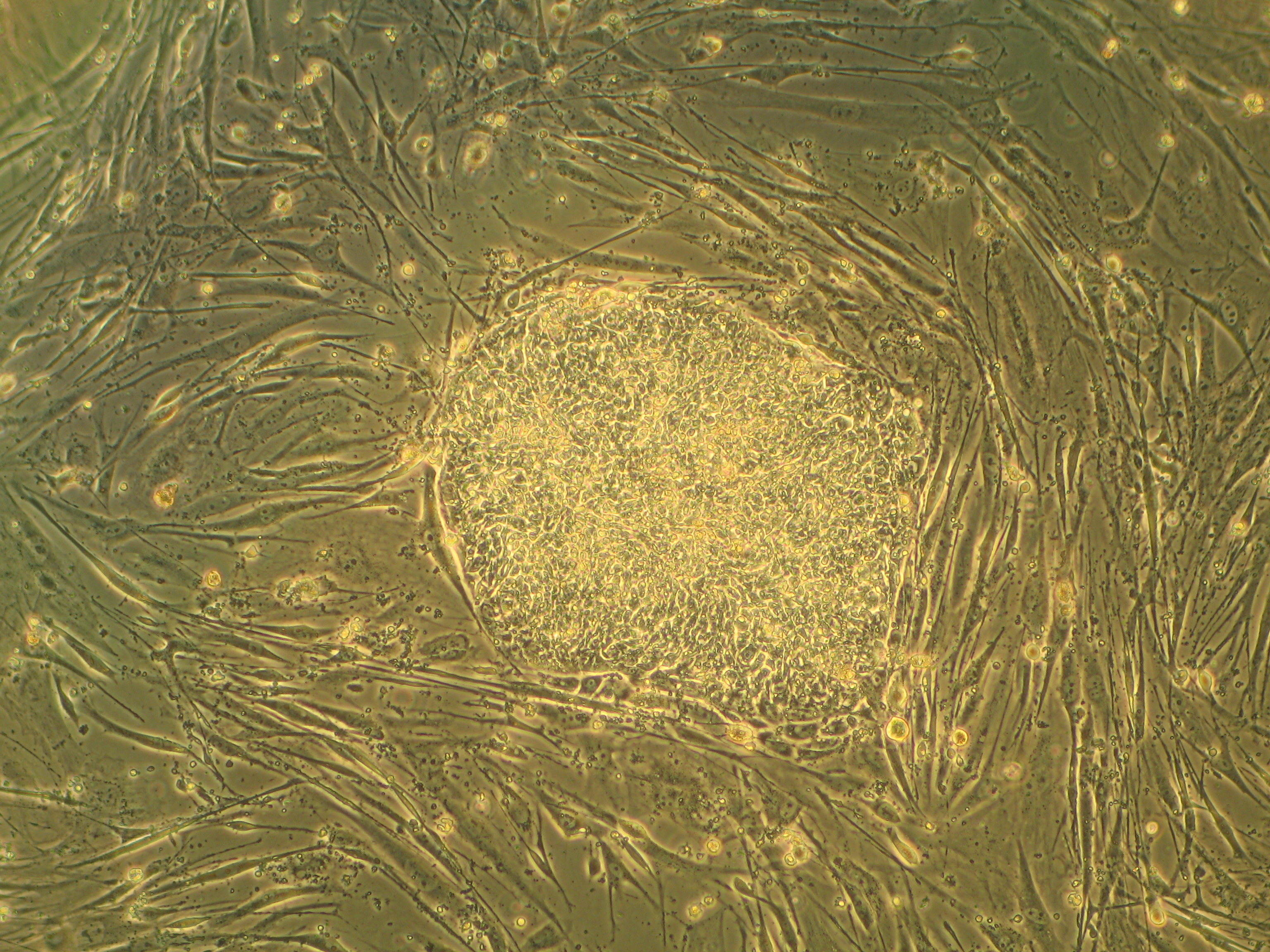
Embryonic stem cells (ESCs) are pluripotent stem cells derived from the inner cell mass of a blastocyst, an early-stage pre-implantation embryo.[1][2] Human embryos reach the blastocyst stage 4–5 days post fertilization, at which time they consist of 50–150 cells. Isolating the inner cell mass (embryoblast) using immunosurgery results in destruction of the blastocyst, a process which raises ethical issues, including whether or not embryos at the pre-implantation stage have the same moral considerations as embryos in the post-implantation stage of development.[3][4]
Researchers are currently focusing heavily on the therapeutic potential of embryonic stem cells, with clinical use being the goal for many laboratories.[2] Potential uses include the treatment of diabetes and heart disease.[2] The cells are being studied to be used as clinical therapies, models of genetic disorders, and cellular/DNA repair. However, adverse effects in the research and clinical processes such as tumors and unwanted immune responses have also been reported.[5]
Concern and controversy[edit]
Adverse effects[edit]
The major concern with the possible transplantation of ESCs into patients as therapies is their ability to form tumors including teratomas.[46] Safety issues prompted the FDA to place a hold on the first ESC clinical trial, however no tumors were observed.
The main strategy to enhance the safety of ESCs for potential clinical use is to differentiate the ESCs into specific cell types (e.g. neurons, muscle, liver cells) that have reduced or eliminated ability to cause tumors. Following differentiation, the cells are subjected to sorting by flow cytometry for further purification. ESCs are predicted to be inherently safer than iPS cells created with genetically integrating viral vectors because they are not genetically modified with genes such as c-Myc that are linked to cancer. Nonetheless, ESCs express very high levels of the iPS inducing genes and these genes including Myc are essential for ESC self-renewal and pluripotency,[47] and potential strategies to improve safety by eliminating c-Myc expression are unlikely to preserve the cells' "stemness". However, N-myc and L-myc have been identified to induce iPS cells instead of c-myc with similar efficiency.[48] Later protocols to induce pluripotency bypass these problems completely by using non-integrating RNA viral vectors such as sendai virus or mRNA transfection.
Techniques and conditions for derivation and culture[edit]
Derivation from humans[edit]
In vitro fertilization generates multiple embryos. The surplus of embryos is not clinically used or is unsuitable for implantation into the patient, and therefore may be donated by the donor with consent. Human embryonic stem cells can be derived from these donated embryos or additionally they can also be extracted from cloned embryos created using a cell from a patient and a donated egg through the process of somatic cell nuclear transfer.[62] The inner cell mass (cells of interest), from the blastocyst stage of the embryo, is separated from the trophectoderm, the cells that would differentiate into extra-embryonic tissue. Immunosurgery, the process in which antibodies are bound to the trophectoderm and removed by another solution, and mechanical dissection are performed to achieve separation. The resulting inner cell mass cells are plated onto cells that will supply support. The inner cell mass cells attach and expand further to form a human embryonic cell line, which are undifferentiated. These cells are fed daily and are enzymatically or mechanically separated every four to seven days. For differentiation to occur, the human embryonic stem cell line is removed from the supporting cells to form embryoid bodies, is co-cultured with a serum containing necessary signals, or is grafted in a three-dimensional scaffold to result.[63]
Derivation from other animals[edit]
Embryonic stem cells are derived from the inner cell mass of the early embryo, which are harvested from the donor mother animal. Martin Evans and Matthew Kaufman reported a technique that delays embryo implantation, allowing the inner cell mass to increase. This process includes removing the donor mother's ovaries and dosing her with progesterone, changing the hormone environment, which causes the embryos to remain free in the uterus. After 4–6 days of this intrauterine culture, the embryos are harvested and grown in in vitro culture until the inner cell mass forms “egg cylinder-like structures,” which are dissociated into single cells, and plated on fibroblasts treated with mitomycin-c (to prevent fibroblast mitosis). Clonal cell lines are created by growing up a single cell. Evans and Kaufman showed that the cells grown out from these cultures could form teratomas and embryoid bodies, and differentiate in vitro, all of which indicating that the cells are pluripotent.[52]
Gail Martin derived and cultured her ES cells differently. She removed the embryos from the donor mother at approximately 76 hours after copulation and cultured them overnight in a medium containing serum. The following day, she removed the inner cell mass from the late blastocyst using microsurgery. The extracted inner cell mass was cultured on fibroblasts treated with mitomycin-c in a medium containing serum and conditioned by ES cells. After approximately one week, colonies of cells grew out. These cells grew in culture and demonstrated pluripotent characteristics, as demonstrated by the ability to form teratomas, differentiate in vitro, and form embryoid bodies. Martin referred to these cells as ES cells.[53]
It is now known that the feeder cells provide leukemia inhibitory factor (LIF) and serum provides bone morphogenetic proteins (BMPs) that are necessary to prevent ES cells from differentiating.[64][65] These factors are extremely important for the efficiency of deriving ES cells. Furthermore, it has been demonstrated that different mouse strains have different efficiencies for isolating ES cells.[66] Current uses for mouse ES cells include the generation of transgenic mice, including knockout mice. For human treatment, there is a need for patient specific pluripotent cells. Generation of human ES cells is more difficult and faces ethical issues. So, in addition to human ES cell research, many groups are focused on the generation of induced pluripotent stem cells (iPS cells).[67]
Potential methods for new cell line derivation[edit]
On August 23, 2006, the online edition of Nature scientific journal published a letter by Dr. Robert Lanza (medical director of Advanced Cell Technology in Worcester, MA) stating that his team had found a way to extract embryonic stem cells without destroying the actual embryo.[68] This technical achievement would potentially enable scientists to work with new lines of embryonic stem cells derived using public funding in the US, where federal funding was at the time limited to research using embryonic stem cell lines derived prior to August 2001. In March, 2009, the limitation was lifted.[69]
Human embryonic stem cells have also been derived by somatic cell nuclear transfer (SCNT).[70][71] This approach has also sometimes been referred to as "therapeutic cloning" because SCNT bears similarity to other kinds of cloning in that nuclei are transferred from a somatic cell into an enucleated zygote. However, in this case SCNT was used to produce embryonic stem cell lines in a lab, not living organisms via a pregnancy. The "therapeutic" part of the name is included because of the hope that SCNT produced embryonic stem cells could have clinical utility.