Benign prostatic hyperplasia
Benign prostatic hyperplasia (BPH), also called prostate enlargement, is a noncancerous increase in size of the prostate gland.[1] Symptoms may include frequent urination, trouble starting to urinate, weak stream, inability to urinate, or loss of bladder control.[1] Complications can include urinary tract infections, bladder stones, and chronic kidney problems.[2]
Benign prostatic hyperplasia
Frequent urination, trouble starting to urinate, weak stream, inability to urinate, loss of bladder control[1]
Age over 40[1]
Unclear[1]
Family history, obesity, type 2 diabetes, not enough exercise, erectile dysfunction[1]
Based on symptoms and examination after ruling out other possible causes[2]
Alpha blockers such as terazosin, 5α-reductase inhibitors such as finasteride[1]
105 million affected globally (2015)[3]
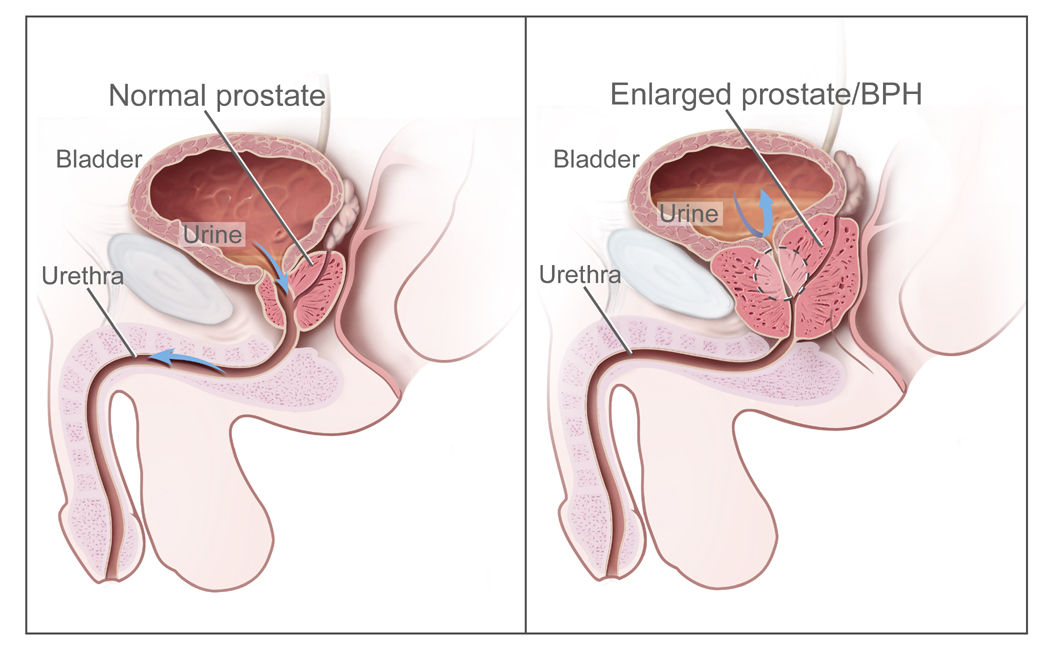
The cause is unclear.[1] Risk factors include a family history, obesity, type 2 diabetes, not enough exercise, and erectile dysfunction.[1] Medications like pseudoephedrine, anticholinergics, and calcium channel blockers may worsen symptoms.[2] The underlying mechanism involves the prostate pressing on the urethra and thereby making it difficult to pass urine out of the bladder.[1] Diagnosis is typically based on symptoms and examination after ruling out other possible causes.[2]
Treatment options include lifestyle changes, medications, a number of procedures, and surgery.[1][2] In those with mild symptoms, weight loss, exercise, and decreasing caffeine intake are recommended, although the quality of the evidence for exercise is low.[2][4] In those with more significant symptoms, medications may include alpha blockers such as terazosin or 5α-reductase inhibitors such as finasteride.[1] Surgical removal of part of the prostate may be carried out in those who do not improve with other measures.[2] Some herbal medicines that have been studied, such as saw palmetto, have not been shown to help.[2] Other herbal medicines somewhat effective at improving urine flow include beta-sitosterol[5] from Hypoxis rooperi (African star grass), pygeum (extracted from the bark of Prunus africana),[6] pumpkin seeds (Cucurbita pepo), and stinging nettle (Urtica dioica) root.[7]
About 105 million men are affected globally.[3] BPH typically begins after the age of 40.[1] Half of males age 50 and over are affected.[2] After the age of 80, that figure climbs to as high as about 90% of males affected.[8][9][1] Although prostate specific antigen levels may be elevated in males with BPH, the condition does not increase the risk of prostate cancer.[10]
Causes[edit]
Hormones[edit]
Most experts consider androgens (testosterone and related hormones) to play a permissive role in the development of BPH. This means that androgens must be present for BPH to occur, but do not necessarily directly cause the condition. This is supported by evidence suggesting that castrated boys do not develop BPH when they age. In an unusual study of 26 eunuchs from the palace of the Qing dynasty still living in Beijing in 1960, the prostate could not be felt in 81% of the studied eunuchs.[21] The average time since castration was 54 years (range, 41–65 years). On the other hand, some studies suggest that administering exogenous testosterone is not associated with a significant increase in the risk of BPH symptoms, so the role of testosterone in prostate cancer and BPH is still unclear. Further randomized controlled trials with more participants are needed to quantify any risk of giving exogenous testosterone.[22]
Dihydrotestosterone (DHT), a metabolite of testosterone, is a critical mediator of prostatic growth. DHT is synthesized in the prostate from circulating testosterone by the action of the enzyme 5α-reductase, type 2. DHT can act in an autocrine fashion on the stromal cells or in paracrine fashion by diffusing into nearby epithelial cells. In both of these cell types, DHT binds to nuclear androgen receptors and signals the transcription of growth factors that are mitogenic to the epithelial and stromal cells. DHT is ten times more potent than testosterone because it dissociates from the androgen receptor more slowly. The importance of DHT in causing nodular hyperplasia is supported by clinical observations in which an inhibitor of 5α-reductase such as finasteride is given to men with this condition. Therapy with a 5α-reductase inhibitor markedly reduces the DHT content of the prostate and, in turn, reduces prostate volume and BPH symptoms.[23][24]
Testosterone promotes prostate cell proliferation,[25] but relatively low levels of serum testosterone are found in patients with BPH.[26][27] One small study has shown that medical castration lowers the serum and prostate hormone levels unevenly, having less effect on testosterone and dihydrotestosterone levels in the prostate.[28]
Besides testosterone and DHT, other androgens are also known to play a crucial role in BPH development. C
21 11-oxygenated steroids (pregnanes) have been identified are precursors to 11-oxygenated androgens which are also potent agonists for the androgen receptor.[29] Specifically, steroids like 11β-hydroxyprogesterone and 11-ketoprogesterone can be converted to 11-ketodihydrotestosterone, an 11-oxo form of DHT with the same potency. These precursors have also been detected in tissue biopsy samples from patients with BPH, as well as in their serum levels.[30][31][32] Besides that, androgens biosythnesized via a backdoor pathway can contribute to the development of BPH.[30]
While there is some evidence that estrogen may play a role in the cause of BPH, this effect appears to be mediated mainly through local conversion of androgens to estrogen in the prostate tissue rather than a direct effect of estrogen itself.[33] In canine in vivo studies castration, which significantly reduced androgen levels but left estrogen levels unchanged, caused significant atrophy of the prostate.[34] Studies looking for a correlation between prostatic hyperplasia and serum estrogen levels in humans have generally shown none.[27][35]
In 2008, Gat et al. published evidence that BPH is caused by failure in the spermatic venous drainage system resulting in increased hydrostatic pressure and local testosterone levels elevated more than 100 fold above serum levels.[36] If confirmed, this mechanism explains why serum androgen levels do not seem to correlate with BPH and why giving exogenous testosterone would not make much difference.
Diet[edit]
Studies indicate that dietary patterns may affect development of BPH, but further research is needed to clarify any important relationship.[37] Studies from China suggest that greater protein intake may be a factor in development of BPH. Men older than 60 in rural areas had very low rates of clinical BPH, while men living in cities and consuming more animal protein had a higher incidence.[38][39] On the other hand, a study in Japanese-American men in Hawaii found a strong negative association with alcohol intake, but a weak positive association with beef intake.[40] In a large prospective cohort study in the US (the Health Professionals Follow-up Study), investigators reported modest associations between BPH (men with strong symptoms of BPH or surgically confirmed BPH) and total energy and protein, but not fat intake.[41] There is also epidemiological evidence linking BPH with metabolic syndrome (concurrent obesity, impaired glucose metabolism and diabetes, high triglyceride levels, high levels of low-density cholesterol, and hypertension).[42]
Degeneration[edit]
Benign prostatic hyperplasia is an age-related disease. Misrepair-accumulation aging theory[43] suggests that development of benign prostatic hyperplasia is a consequence of fibrosis and weakening of the muscular tissue in the prostate.[44] The muscular tissue is important in the functionality of the prostate, and provides the force for excreting the fluid produced by prostatic glands. However, repeated contractions and dilations of myofibers will unavoidably cause injuries and broken myofibers. Myofibers have a low potential for regeneration; therefore, collagen fibers need to be used to replace the broken myofibers. Such misrepairs make the muscular tissue weak in functioning, and the fluid secreted by glands cannot be excreted completely. Then, the accumulation of fluid in glands increases the resistance of muscular tissue during the movements of contractions and dilations, and more and more myofibers will be broken and replaced by collagen fibers.[45]
Micrograph showing nodular hyperplasia (left off center) of the prostate from a transurethral resection of the prostate (TURP). H&E stain.

Microscopic examination of different types of prostate tissues (stained with immunohistochemical techniques): A. Normal (non-neoplastic) prostatic tissue (NNT). B. Benign prostatic hyperplasia. C. High-grade prostatic intraepithelial neoplasia. D. Prostatic adenocarcinoma (PCA).
