Hodgkin lymphoma
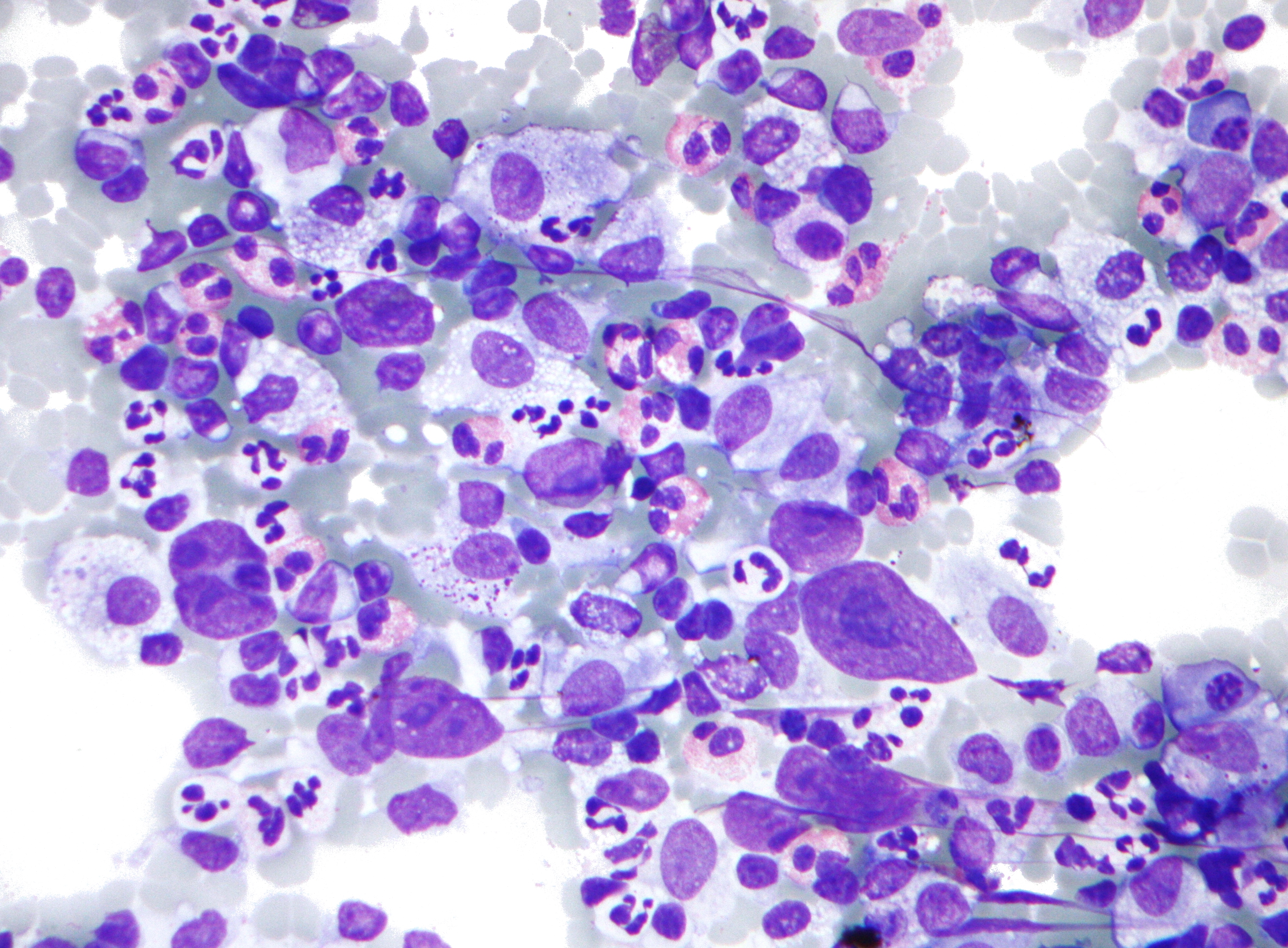
Hodgkin lymphoma (HL) is a type of lymphoma in which cancer originates from a specific type of white blood cell called lymphocytes, where multinucleated Reed–Sternberg cells (RS cells) are present in the patient's lymph nodes.[2][8] The condition was named after the English physician Thomas Hodgkin, who first described it in 1832.[9][10] Symptoms may include fever, night sweats, and weight loss.[2] Often, nonpainful enlarged lymph nodes occur in the neck, under the arm, or in the groin.[2] Persons affected may feel tired or be itchy.[2]
Hodgkin lymphoma
Hodgkin's lymphoma, Hodgkin's disease[1]
Hematology and oncology
Fever, night sweats, weight loss, nonpainful enlarged lymph nodes[2]
Epstein–Barr virus, family history, HIV/AIDS[2][3]
Five-year survival rate 88% (US)[5]
574,000 (affected during 2015)[6]
23,900 (2015)[7]
The two major types of Hodgkin lymphoma are classic Hodgkin lymphoma and nodular lymphocyte-predominant Hodgkin lymphoma.[5] About half of cases of Hodgkin lymphoma are due to Epstein–Barr virus (EBV) and these are generally the classic form.[3][11] Other risk factors include a family history of the condition and having HIV/AIDS.[2][3] Diagnosis is conducted by confirming the presence of cancer and identifying RS cells in lymph node biopsies.[2] The virus-positive cases are classified as a form of the Epstein–Barr virus-associated lymphoproliferative diseases.[12]
Hodgkin lymphoma may be treated with chemotherapy, radiation therapy, and stem-cell transplantation.[4] The choice of treatment often depends on how advanced the cancer has become and whether or not it has favorable features.[4] If the disease is detected early, a cure is often possible.[9] In the United States, 88% of people diagnosed with Hodgkin lymphoma survive for five years or longer.[5] For those under the age of 20, rates of survival are 97%.[13] Radiation and some chemotherapy drugs, however, increase the risk of other cancers, heart disease, or lung disease over the subsequent decades.[9]
In 2015, about 574,000 people globally had Hodgkin lymphoma, and 23,900 (4.2%) died.[6][7] In the United States, 0.2% of people are affected at some point in their life.[5] Most people are diagnosed with the disease between the ages of 20 and 40.[5]
People with Hodgkin lymphoma may present with these symptoms:
Treatment of Hodgkin's disease has been improving over the past few decades. Recent trials that have made use of new types of chemotherapy have indicated higher survival rates than have previously been seen. In a 2007 European trial, the five-year survival rate for those people with a favorable prognosis (FFP) was 98%, while that for people with worse outlooks was at least 85%.[66]
In 1998, an international effort[67] identified seven prognostic factors that accurately predict the success rate of conventional treatment in people with locally extensive or advanced-stage Hodgkin lymphoma. Freedom from progression (FFP) at five years was directly related to the number of factors present in a person. The five-year FFP for people with zero factors is 84%. Each additional factor lowers the five-year FFP rate by 7%, such that the five-year FFP for a person with five or more factors is 42%.[68]
The adverse prognostic factors identified in the international study are:
Other studies have reported the following to be the most important adverse prognostic factors: mixed-cellularity or lymphocyte-depleted histologies, male sex, large number of involved nodal sites, advanced stage, age of 40 years or more, the presence of B symptoms, high erythrocyte sedimentation rate, and bulky disease (widening of the mediastinum by more than one third, or the presence of a nodal mass measuring more than 10 cm in any dimension.)[69]
More recently, the use of positron emission tomography (PET) early after commencing chemotherapy has demonstrated to have powerful prognostic ability.[70] This enables assessment of an individual's response to chemotherapy as the PET activity switches off rapidly in people who are responding. In this study,[70] after two cycles of ABVD chemotherapy, 83% of people were free of disease at 3 years if they had a negative PET versus only 28% in those with positive PET scans. This prognostic method improves on FFP estimates based on the seven conventional factors. Several trials are underway to see if PET-based risk adapted response can be used to improve a person's outcomes by changing chemotherapy early in people who are not responding.
The evidence is very uncertain about the effect of negative (= good prognosis) or positive (= bad prognosis) interim PET scan results for patients with a Hodgkin's lymphoma on the progression-free survival. Negative interim PET scan results may result in an increase in progression-free survival compared if the adjusted result was measured. Negative interim PET scan results probably result in a large increase in the overall survival compared to those with a positive interim PET scan result,[43]