
Ectopic pregnancy
Ectopic pregnancy is a complication of pregnancy in which the embryo attaches outside the uterus.[5] Signs and symptoms classically include abdominal pain and vaginal bleeding, but fewer than 50 percent of affected women have both of these symptoms.[1] The pain may be described as sharp, dull, or crampy.[1] Pain may also spread to the shoulder if bleeding into the abdomen has occurred.[1] Severe bleeding may result in a fast heart rate, fainting, or shock.[5][1] With very rare exceptions, the fetus is unable to survive.[6]
Ectopic pregnancy
EP, eccyesis, extrauterine pregnancy, EUP, tubal pregnancy (when in fallopian tube)
Pelvic inflammatory disease, tobacco smoking, prior tubal surgery, history of infertility, use of assisted reproductive technology[2]
Blood tests for human chorionic gonadotropin (hCG), ultrasound[1]
methotrexate, surgery[2]
Mortality 0.2% (developed world), 2% (developing world)[4]
~1.5% of pregnancies (developed world)[5]
Overall, ectopic pregnancies annually affect less than 2% of pregnancies worldwide.[5]
Risk factors for ectopic pregnancy include pelvic inflammatory disease, often due to chlamydia infection; tobacco smoking; endometriosis; prior tubal surgery; a history of infertility; and the use of assisted reproductive technology.[2] Those who have previously had an ectopic pregnancy are at much higher risk of having another one.[2] Most ectopic pregnancies (90%) occur in the fallopian tube, which are known as tubal pregnancies,[2] but implantation can also occur on the cervix, ovaries, caesarean scar, or within the abdomen.[1] Detection of ectopic pregnancy is typically by blood tests for human chorionic gonadotropin (hCG) and ultrasound.[1] This may require testing on more than one occasion.[1] Other causes of similar symptoms include: miscarriage, ovarian torsion, and acute appendicitis.[1]
Prevention is by decreasing risk factors such as chlamydia infections through screening and treatment.[7] While some ectopic pregnancies will miscarry without treatment,[2] the standard treatment for ectopic pregnancy is a procedure to either remove the embryo from the fallopian tube or to remove the fallopian tube all together. The use of the medication methotrexate works as well as surgery in some cases.[2] Specifically it works well when the beta-HCG is low and the size of the ectopic is small.[2] Surgery such as a salpingectomy is still typically recommended if the tube has ruptured, there is a fetal heartbeat, or the woman's vital signs are unstable.[2] The surgery may be laparoscopic or through a larger incision, known as a laparotomy.[5] Maternal morbidity and mortality are reduced with treatment.[2]
The rate of ectopic pregnancy is about 11 to 20 per 1,000 live births in developed countries, though it may be as high as 4% among those using assisted reproductive technology.[5] It is the most common cause of death among women during the first trimester at approximately 6-13% of the total.[2] In the developed world outcomes have improved while in the developing world they often remain poor.[7] The risk of death among those in the developed world is between 0.1 and 0.3 percent while in the developing world it is between one and three percent.[4] The first known description of an ectopic pregnancy is by Al-Zahrawi in the 11th century.[7] The word "ectopic" means "out of place".[8]
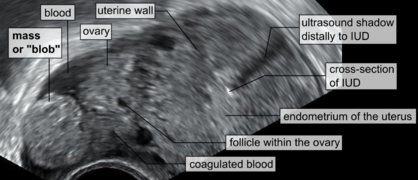
Transvaginal ultrasonography of an ectopic pregnancy, showing the field of view in the following image

A "blob sign", which consists of the ectopic pregnancy. The ovary is distinguished from it by having follicles, whereof one is visible in the field. This patient had an intrauterine device (IUD) with progestogen, whose cross-section is visible in the field, leaving an ultrasound shadow distally to it.

Treatment[edit]
Expectant management[edit]
Most women with a PUL are followed up with serum hCG measurements and repeat TVS examinations until a final diagnosis is confirmed.[5] Low-risk cases of PUL that appear to be failing pregnancies may be followed up with a urinary pregnancy test after two weeks and get subsequent telephone advice.[5] Low-risk cases of PUL that are likely intrauterine pregnancies may have another TVS in two weeks to access viability.[5] High-risk cases of PUL require further assessment, either with a TVS within 48 h or additional hCG measurement.[5]
Medical[edit]
Early treatment of an ectopic pregnancy with methotrexate is a viable alternative to surgical treatment[56] which was developed in the 1980s.[57] If administered early in the pregnancy, methotrexate terminates the growth of the developing embryo; the developing embryo may then be either resorbed by the woman's body or pass with a menstrual period. Contraindications include liver, kidney, or blood disease, as well as an ectopic embryonic mass > 3.5 cm.
Also, it may lead to the inadvertent termination of an undetected intrauterine pregnancy, or severe abnormality in any surviving pregnancy.[5] Therefore, it is recommended that methotrexate should only be administered when hCG has been serially monitored with a rise less than 35% over 48 hours, which practically excludes a viable intrauterine pregnancy.[5]
For nontubal ectopic pregnancy, evidence from randomised clinical trials in women with CSP is uncertain regarding treatment success, complications and side effects of methotrexate compared with surgery (uterine arterial embolization or uterine arterial chemoembolization).[58]
The United States uses a multi dose protocol of methotrexate (MTX) which involves four doses of intramuscular along with an intramuscular injection of folinic acid to protect cells from the effects of the drugs and to reduce side effects. In France, the single dose protocol is followed, but a single dose has a greater chance of failure.[59]
Society and culture[edit]
Salpingectomy as a treatment for ectopic pregnancy is one of the common cases when the principle of double effect can be used to justify accelerating the death of the embryo by doctors and patients opposed to outright abortions.[73]
In the Catholic Church, there are moral debates on certain treatments. A significant number of Catholic moralists consider use of methotrexate and the salpingostomy procedure to be not "morally permissible" because they destroy the embryo; however, situations are considered differently in which the mother's health is endangered, and the whole fallopian tube with the developing embryo inside is removed.[74][75]
Organisations exist that provide information and support to help those who experience ectopic pregnancy. Studies show that people can experience post-traumatic stress, depression, and anxiety for which they would need specialist therapies.[76] Partners can also experience post-traumatic stress.[77]
Live birth[edit]
There have been cases where ectopic pregnancy lasted many months and ended in a live baby delivered by laparotomy.
In July 1999, Lori Dalton gave birth by caesarean section in Ogden, Utah, United States, to a healthy baby girl, Saige, who had developed outside of the uterus. Previous ultrasounds had not discovered the problem. "[Dalton]'s delivery was slated as a routine Caesarean birth at Ogden Regional Medical Center in Utah. When Dr. Naisbitt performed Lori's Caesarean, he was astonished to find Saige within the amniotic membrane outside the womb ... ."[78] "But what makes this case so rare is that not only did mother and baby survive—they're both in perfect health. The father, John Dalton took home video inside the delivery room. Saige came out doing extremely well because even though she had been implanted outside the womb, a rich blood supply from a uterine fibroid along the outer uterus wall had nourished her with a rich source of blood."[79]
In September 1999 an English woman, Jane Ingram (age 32) gave birth to triplets: Olivia, Mary and Ronan, with an extrauterine fetus (Ronan) below the womb and twins in the womb. All three survived. The twins in the womb were taken out first.[80]
On May 29, 2008, an Australian woman, Meera Thangarajah (age 34), who had an ectopic pregnancy in the ovary, gave birth to a healthy full term 6 pound 3 ounce (2.8 kg) baby girl, Durga, via Caesarean section. She had no problems or complications during the 38‑week pregnancy.[81][82]
Leg of fetal lamb appearing out of the uterus during caesarean section

External view of fetal sac, necrotic distal part

Internal view of fetal sac, before resection of distal necrotic part

Internal view of fetal sac. The necrotic distal part is to the left.

External side of fetal sac, proximal end, with ovary and uterine horn

Resected distal part of fetal sac, with attached placenta

Ectopic gestation exists in mammals other than humans. In sheep, it can go to term, with mammary preparation to parturition, and expulsion efforts. The fetus can be removed by caesarean section. Pictures of caesarian section of a euthanized ewe, five days after parturition signs.