Intracranial hemorrhage
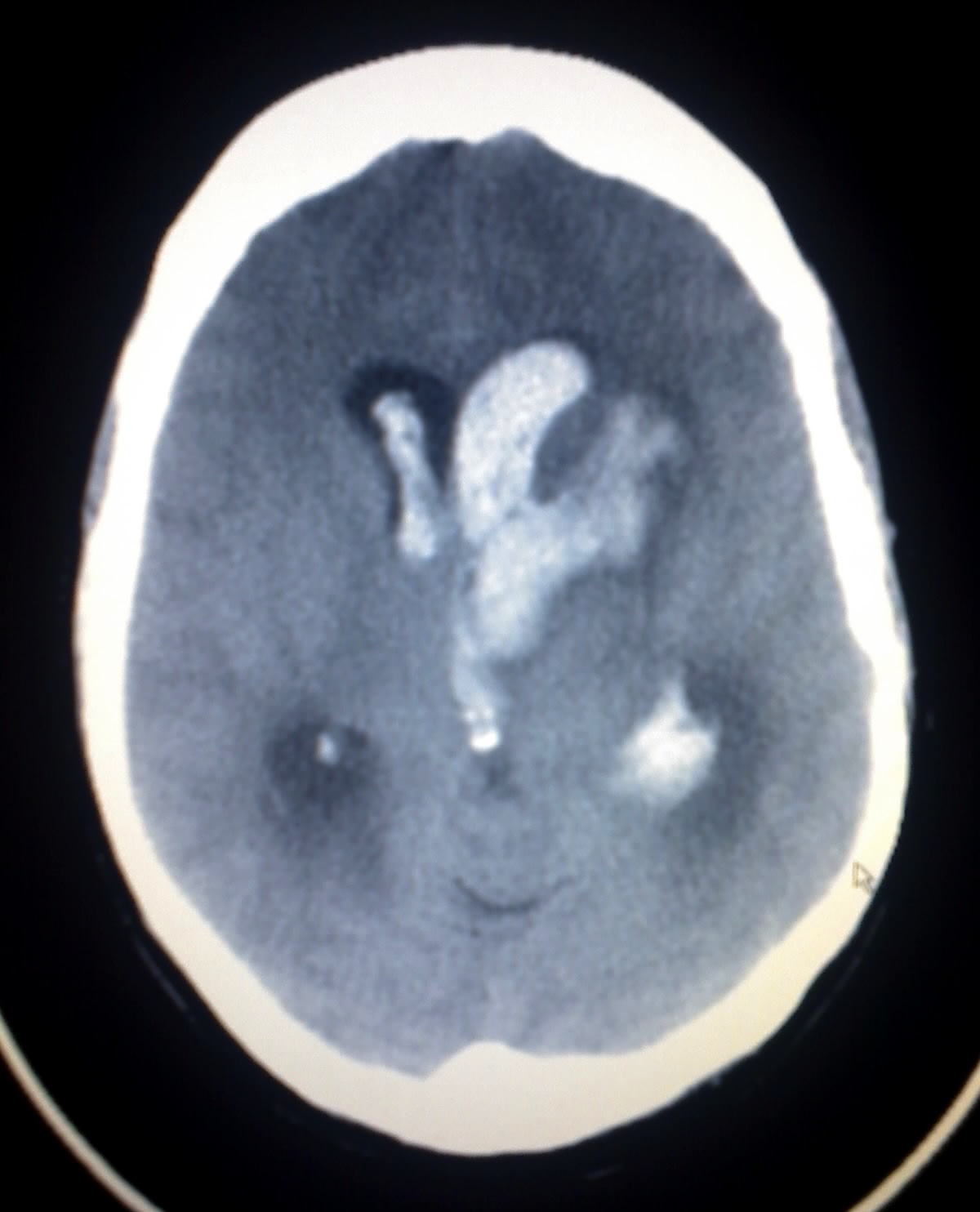
Intracranial hemorrhage (ICH), also known as intracranial bleed, is bleeding within the skull.[1] Subtypes are intracerebral bleeds (intraventricular bleeds and intraparenchymal bleeds), subarachnoid bleeds, epidural bleeds, and subdural bleeds.[2]
Intracranial hemorrhage
Same symptoms as ischemic stroke, but unconsciousness, headache, nausea, stiff neck, and seizures are more often in brain hemorrhages than ischemic strokes
Coma, persistent vegetative state, cardiac arrest (when bleeding is in the brain stem or is severe), death
Stroke, head injury, ruptured aneurysm
Intracerebral bleeding affects 2.5 per 10,000 people each year.[1]
Signs and symptoms[edit]
Intracranial hemorrhage is a serious medical emergency because the buildup of blood within the skull can lead to increases in intracranial pressure, which can crush delicate brain tissue or limit its blood supply. Severe increases in intracranial pressure (ICP) can cause brain herniation, in which parts of the brain are squeezed past structures in the skull.
Symptoms include severe headache, nausea/vomiting, seizures, dizziness or lightheadedness or vertigo, one-sided facial drooping, one-sided numbness, weakness, tingling, or paralysis, speech problems, blindness, deafness, memory issues, attention problems, balance problems, coordination problems and decreasing level of consciousness or complete loss of consciousness. Coma and persistent vegetative state can result from intracranial hemorrhage.
Brain stem hemorrhage may cause additional symptoms such as shortness of breath, dysphagia (difficulty swallowing), chewing problems, abnormal heart rate, and irregular heartbeat. Brain stem hemorrhage can cause cardiac arrest.
Causes[edit]
Trauma is the most common cause of intracranial hemorrhage. It can cause epidural hemorrhage, subdural hemorrhage, and subarachnoid hemorrhage. Other condition such as hemorrhagic parenchymal contusion and cerebral microhemorrhages can also be caused by trauma.[3]
Non-traumatic causes of hemorrhage includes: hypertension, cerebral amyloid angiopathy, hemorrhagic conversion of ischemic infarction, cerebral aneurysms, dural arteriovenous fistulae, cerebral venous sinus thrombosis, cerebral vasculitis and mycotic aneurysm.[3]
More than half of all cases of intracranial hemorrhage are the result of hypertension.
Management[edit]
For those who is already on blood thinners such as aspirin or clopidogrel for prevention of myocardial infarction or stroke, traumatic intracranial hemorrhage should prompt the use of platelet function assays (PFA-100) to assess the effect of these antiplalelet agents. After that, plateletpheresis can be started to increase the aggregation of platelets, thus stopping the intracranial bleed. In those with impaired kidney functions, desmopressin or cryoprecipitate can be used instead.[11]
From limited observational data, it may be relatively safe to restart blood thinners after an ICH as it is asscoated with reduced thromboembolic complications with similar risk of recurrent hemorrhage when compared to those did not start blood thinners after an ICH.[12]